Anjali Jameson is Senior Vice President of Product at One Medical, a nationwide primary care organization that offers 24/7 virtual, on-demand care. Early in her career, she worked as VP of Product at The Go Game before joining Apple as an MBA intern. Anjali then joined Apple’s Online Store division full-time and worked on their online store mobile experiences. She later transitioned into product leadership at various healthcare companies, including UnitedHealth Group, Zipongo, Habit, and, now, OneMedical.

In our conversation, Anjali talks about “humanizing” the healthcare system and how her team’s work feels personal because they’re solving issues that they or their loved ones have faced. She discusses key differences in building healthcare products versus regular tech products, such as how things get paid for, regulations and licensing, and the complexity of data and connecting into the system. Anjali also shares the challenge of scaling when the product’s users aren’t actually the ones who bring in revenue for the company.
I have been a One Medical member for over a decade and I don’t think I’ve found a care organization that can do what it does. My husband and I were going to India and needed to get all our travel care done. There are many things we had to do — vaccines, medications, etc. I went on my One Medical app, answered a few questions, and within an hour, I had prescriptions being sent to a pharmacy and labs being ordered to the nearest One Medical. Everything was taken care of within a day. It’s the convenience aspect — we’ve modernized things that get really frustrating in healthcare and made them very convenient.
We provide on-demand video calls. You can call at midnight or 5 a.m. with time-sensitive questions or needs. And we connect to the system. Across the country, we connect to technologies in hospital systems so that we can do easy referrals, data transfer, etc. Care for our patients is not just what happens within our four walls, we extend past that because no one likes to feel anonymous within the healthcare system. It feels very lonely to leave a doctor’s office and think, “What do I do next?” Behind the scenes, our people and technology connect data and insurance and handle administrative work, among other things to make sure the patient’s care experience feels seamless. I truly haven’t found anything better for myself or my family.
I had a three-month internship at Apple when I was getting my business degree. I was asked to return to run their mobile web platform, which is hilarious because this was back in the day when people had mobile web initiatives. Thankfully, that was a very short era, but I was responsible for Apple’s online store mobile web experience. Within a few months of that, I took over responsibility for all the mobile platforms. Apple’s online store, at the time, was incredibly design-driven so there was one of me and eight or 10 designers.
Because of my role on mobile, any big initiative that hit the store would hit me and my world. We expanded the app access to eight new countries in all new languages and payment types. Launching buy online, pick up in-store was another big one. This was my first taste of the processes at a very large company. Everything was big. My product requirements documents would be scrolls. Everything had to be fully baked. Release plans were super significant. To release an update, the online store would go dark for several hours overnight. We’d shut down the store and do overnighters at the office, where we get it all ready and bring the store back up again.
It was a very different experience. The most rewarding part was that they had no one in the online store who was responsible at that time for accessibility. So, on top of the mobile stuff, they asked me to take on accessibility. I represented the online store midway through my time at Apple, and then I worked really closely with some of the most brilliant accessibility minds across Apple — they were leading the charge in consumer devices on accessibility. Working with them on how to improve accessibility across Apple was probably my favorite part of that role.
There are three areas that are very different from traditional tech. One is how things get paid for. In B2B, you build a product for businesses, businesses like it, and they pay for it. In B2C, you build a product, consumers like it, they buy it, they pay for it. In healthcare, it’s super circuitous. It is a very complex system of how you get paid. Who you’re building for is not generally who is paying for it.
The second is regulations and licensing. Health care is a highly regulated space. Every state has its own rules for everything from licensure to telehealth rules to billing rules. For example, state-by-state rules. Instead of trying to hide all of that complexity, you want to surface a little bit of it. Because otherwise, people don’t understand why they’re seeing something different in one state versus another. In product, we often want to hide all the complexity, but there’s some layer of friction that’s important so we can educate people and help avoid surprises.
The final thing is the complexity of data and connecting to the system. Your health data is disparate — it’s in many places and in many formats. Being able to gather comprehensive data for our patients is something that we’ve tried to solve at One Medical because we want to understand the whole person, not just who they are when they’re in front of us. Improving data interoperability and accessibility is a lot of work. It’s taken a lot of investment and a lot of work in earnest, and we’ve made a lot of progress but have more to do.
The short of it is we connect to many hospital systems to pull in data. We also connect to HIEs, or health information exchanges, where health data from across the spectrum of providers to health plans from all over the country gets pulled into one place. The part that’s hard, but not insurmountable, is interpreting it all. If we pull in millions of documents, how do we process all that information to timely and relevantly inform care for our members? We are excited about leveraging machine learning for this purpose — to aid us in processing health documents and organize data into the right places.
Some of it is just knowing who we are. We are a membership-based practice, and people used to traditional health care often don’t intuitively understand what we do. People aren’t out walking around thinking, “I need a healthcare membership.” Explaining what we do, why we do it, and why there is a small cost to join is different. There are no real comparisons out in the market, even today. We have a large percentage of new members coming in through word-of-mouth referrals, so when we go to new markets, we recognize the importance of getting that flywheel of referrals started.
In healthcare, operational scale is critical and isn’t easy to do. I think we’ve all seen startups and midsize companies build beautiful, creative, user-forward healthcare experiences or wellness products. But within healthcare, users aren’t usually the ones who are responsible for paying the bills. That makes things incredibly challenging — you can build an incredible user experience and not be able to actually get to operational scale because you don’t have the funding to do so. I’ve learned that you have to think about creating incredible user experiences with as little waste as possible.
That means testing all assumptions. That’s good product management anywhere, but it’s so critical in healthcare because you have few resources to waste. Also, as you’re building and growing, you have to build teams, processes, and roadmaps that, while focused on great user experience, also acknowledge and build around the healthcare system. That often works against great user experience.
To do that well and to sit in that middle space is not easy for most of us. And we do it because the healthcare system in this country is awful. Many of us are very mission-driven to fix this, but we sit in that crazy buffer zone of creating incredible user experience while also acknowledging that you’re building within a healthcare system that can work against that.
When we think about building products within healthcare, my whole team understands where they sit within this challenging ecosystem. We spend over $4.5 trillion on healthcare in the US. Anytime you’re building healthcare products in this system, you are touching a number of those complexities. We try to break some of those apart to tackle them. Every leader on my team runs different parts of the portfolio and is responsible for different stakeholders within the healthcare system.
The leader of our provider and care team experiences is responsible for working with our providers, operational leaders, and the different stakeholders that contribute to driving the success of our business models — commercial payers, government, enterprise, etc. Our leader over all of our data and interoperability is responsible for connecting into the healthcare system. She works closely with hospital systems, other provider organizations, and payer and government as well.
Every product leader and their associated teams are working very closely with stakeholders across the org. At times, some of them work with external organizations and industry groups to help define standards and establish thought leadership on regulations. We work with many of the players across the healthcare system to make a model in primary care that works.
The main thing I’ve said before to folks who are considering it is that you will feel frustrated a lot, but you will feel like you’re working on something that really matters. As product managers, we work a lot of hours. And we have to do a lot of stakeholder management. But at the end of the day, we can actually see the impact we are making. We can go into our clinics and shadow providers to see the care that we’re enabling. The number of people who have teared up about it, it’s different than working in any other industry. It is personal. Frustrations with the current state of health care are something we’ve all experienced, and having an opportunity to solve these hard problems is deeply motivating.
That is the best part about working in healthcare. And the most challenging part is that, no matter how fast you want to go or how small the company is, there are more trade-offs that you have to make at each step of the product development lifecycle to get things done that meet the consumer need and is economically sustainable.
We look at all the classic metrics like NPS, customer satisfaction scores, and what we’re hearing anecdotally from customer support, our virtual medical team, etc. We measure satisfaction scores in offices and with providers. We’re also looking at access, which refers to our providers’ availability to see patients, because if there’s no access in a certain market, that would be our biggest dissatisfier. We look at the third next available appointment and same-day appointments to make sure we have access in every market and every location.
Our technology org along with most folks on our teams across the organization, go to what we call Gemba, or rounds. And rounds are every month — go into a clinic, sit and shadow for an hour, and then everyone comes back together over Zoom and talks about what we saw that worked well, what didn’t, and what maybe needs to be changed. It’s a chance to humanize what we do and see the technology in action. That helps us catch things that, while they may not serve us in the metrics, you can see as problems. And so, that’s a great part about building technology for in-person interactions, you can actually watch them happen and see what works.
The short of it is scaling primary care and how we can work to operationally scale this incredible service to more people. Our quality scores are excellent and the on-demand care that we can provide is oftentimes within a few minutes, if not, within a couple of hours. All of those things feel like if we can get it to more members, we will be making healthcare more accessible, improving population health, and lowering the cost of care.
When it comes to actual individual capabilities, there’s a lot of excitement around AI, and for good reason. I’m really excited about the opportunity to use AI to remove the increasing number of administrative tasks and the burdens weighing down care teams and providers so they can focus on providing human-centered care. We’re looking at things like understanding external health records so that providers better understand the patient before providing care to them.
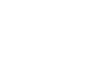
LogRocket identifies friction points in the user experience so you can make informed decisions about product and design changes that must happen to hit your goals.
With LogRocket, you can understand the scope of the issues affecting your product and prioritize the changes that need to be made. LogRocket simplifies workflows by allowing Engineering, Product, UX, and Design teams to work from the same data as you, eliminating any confusion about what needs to be done.
Get your teams on the same page — try LogRocket today.
Learn how product managers can use human-in-the-loop AI to manage decision risk, set oversight, and keep ownership and accountability human.
Learn how to choose and adapt product management frameworks based on your product stage, constraints, problem type, and business context.

Learn when streaks improve retention, when they create fragile engagement, and how PMs can design healthier systems around user progress.

A technical debt register brings transparency and clarity as to what type and how much debt you have and can be used to monitor and review your debt ratio.