Rob Helton is SVP, Product at WebPT, a practice experience management platform for rehab therapy professionals. After getting his doctorate in physical therapy, he started his career as a physical therapist at Moss Rehab before transitioning to Allied Services. From there, Rob became general manager of rehabilitation at Cerner Corporation before moving into product management. Before his current role at WebPT, he served in leadership positions at Oracle and Ontada.

In our conversation, Rob talks about the potential for technology to impact the bottom line across the healthcare industry. He discusses the importance of combining AI and technology with human intuition, as well as the need to consistently push for better product outcomes.
Everybody wants to ship code every moment they can. That’s one of the mantras of the industry. I have friends who go to production twice a day, and I know that small, iterative chunks are the right way to endure your business. On the flip side, for healthcare, in some cases, you can do that, but it’s not very common. Especially when we’re talking about electronic medical records, EMRs, and our users — while they are some of the most educated people in the world, they’re still clinicians. They experience extreme change fatigue because they use our system so regularly.
Even with things like moving buttons or changing functionality without an obvious release creates a lot of frustration. We also have a lot of thought processes around iterative adjustments. We have to continuously test and ensure that we have regulatory compliance, as well as patient safety measures and financial coverage for anything that we do. We want to keep testing as we produce the code and put it out.
We’ve found that, at least for the part of healthcare we’re in, we should ship larger chunks of functionality that show the end-to-end picture in the workflow versus small pieces. This is because it’s easier to adopt, we have a better impact, and it’s the only way we can guarantee regulatory, financial, and patient safety.
We want to have as much automated code coverage as possible for anything that we do, and this extends beyond errors. We also have to have test coverage — whether it’s manual or automated — for those regulatory impacts, financial impacts, and patient safety. I can’t compare this to other industries, but for us, this means that we have to have a large set of test data, whether it’s synthetic or masked.
Managing the test data becomes its own challenge in the process because as we evolve the functionality, we have to evolve the test data. A lot of times, we have to create these large data sets to test functionality that we haven’t even released yet, or don’t have any example data from.
At WebPT, we have a large product suite. We have many products that we aim for our partners to use as their end-to-end solutions for outpatient physical, occupational, and speech therapy. Because of this, change fatigue doesn’t just occur for one product — it lies in how the products work together. For example, say that you go into Microsoft Office every day. This is a likely scenario for many people, so imagine that suddenly, Excel and Word had completely non-aligned functionality. Now, you can’t cut and paste anymore between your products.
Imagine how frustrating that would be for a user. It’s not just purity internal to the product, it’s the purity across the ecosystem.
When I work with other product people across other industries, the push is always for an MVP. How quickly can you launch your MVP? There’s even the question of, “What’s your cycle time from idea to innovation to release?” In healthcare, especially if you’re affecting a critical use product like medication ordering, there is no MVP for that. It would be almost impossible to have all medications that anybody could order, go through drug dose and allergy checking, electronic integration, ePrescribe, etc. There’s a whole stack of functionality.
That’s why MVPs don’t make a lot of sense in this industry — the basement requirements are so exceedingly high that you can sometimes spend years before you reach a solution ready to displace anything. I’ve found that many people think that EMRs are a new technology. They’re something that just happened in the last decade, but the reality is many of the electronic medical records that exist come from decades ago. Forcing the modernization of technology that’s 20–30 years old is a big struggle. So what do you do to combat that?
I have a belief that if you’re in a similar situation, you have to be consistently in the process of reinventing yourself in a meaningful way. Whenever you think about technical debt, that doesn’t just mean OS or architecture upgrades — it means always chipping away at your current product and trying to update it as you go. You have to prioritize automating and updating things. How can you change pieces and increase the functionality without just iterating on the same thing over and over? It’s a very delicate balance. Everybody wants their EMR to get better.
I think that’s why you see everybody developing AI in healthcare starting in the periphery and moving onwards. They’re starting with models that look at radiographs to find tumors. They’re looking at ambient speech-scribing capabilities for documentation. I am not aware yet of an AI company that said, “Hey, you know what I’m going to do in the next three years? We’re going to replace an EMR.” Because it’s easier to be outside in than it is inside out.
These things are surfacing more and more nowadays. I think that there is an insufficient focus on developer and product tools that utilize AI to help boost team productivity. We’re starting to see them in not just the co-pilots of the world and things that snap into ecosystems. Where is our requirements’ writer software that can take human speech and turn it into requirements, and where is our software that takes those requirements and helps us generate test cases? That is something that is just the pit of human sorrow — the loop is horrifically long!
Where’s the AI that helps us do better synthetic testing and tracing so that we know the performance? Where’s the AI that helps me create synthetic data so that we can do scale loads before we launch something to a hundred thousand users overnight and find out that we are woefully under capacity? Where’s the AI to help me manage incidents? Zero product managers or engineers enjoy their pager duty call at 2:00 a.m., so what technology can help with that?
When I think about those things, the problem that I see is that either it’s really hard or there’s no money in it. Otherwise, somebody in San Francisco tonight is going to have a great idea. Those items would create so much capacity for velocity and functional quality. I don’t think the goal of AI is to replace human beings but to elevate us. That’s what I’m yearning for.
Healthcare today is in a crisis. It’s overly complex. We have super old technology because there haven’t been incentives to modernize. On the flip side, everything that is cool and fit like AI has difficulty incorporating into a regulated industry. I’d go as far as to say that healthcare is the hardest for us to incorporate AI into.
There are really awesome AI applications coming out to combat clinician burnout head-on. Some of the partners that we see in the space are creating ambient AI scribing and listening, which reduces the amount of time that people have to interface with a keyboard. We’re seeing really cool advances in capacity management. That’s helping with managing the top line for our hospital and application systems.
With that, there’s a natural friction. Everybody in the AI space wants to focus on where the money is, and that makes perfect sense. But the broader healthcare ecosystem doesn’t get much of the attention because of that. We’re not elevating healthcare — we’re elevating individuals inside of healthcare. And yes, patient care is improving. We’re helping the bottom line and health organizations stay in business.
What a great question. The obvious and unsatisfying answer is that it’s very hard for humans to know that because of the unknowability of AI. The reason that these models are so successful is that they look at factors that humans don’t correlate with and speculate patients’ impacts and outcomes.
It’s twofold. I refer to one big factor as the sniff test, which means using your human intuition. If you’re going to work with AI, there has to be a baseline ethical training, education, and awareness of how they function and what the reasonable limitations of those models are. You cannot run a healthcare product group where there’s only one person who understands what’s going on and everyone else looks to them as the safeguard. Ethics is a group responsibility.
The other is that, thankfully, we’re starting to see healthcare regulations focus on where AI and clinical decision-making affect our users and patients. The larger U.S. healthcare regulators have started publishing guidelines, transparency, and knowability of AI and healthcare. Essentially, if an AI is making suggestions on the best choices for a patient, it has to be explained in human-readable language appropriate to education level. It also has to explain the selection criteria, factors that went into the analysis, etc.
If you are not thinking about how to elevate your individuals through AI and modern technology, or how to scale your users and what they’re trying to accomplish through AI and modern technology, I don’t think you’ll be in business in five years.
The ability to create products is becoming so rapid because of this technology. We can ideate, innovate, publish, monitor, and scale with AI. If you’re not thinking about how to leverage this technology, you’re going to get out-performed very quickly. Now, is it a necessary baseline? Probably not. Some companies are going to be fine, but if your job is to produce something — especially if you’re consumer-facing — you have to be doing these things. There’s a market expectation now.
Even how you monitor and run your go-to-market has changed extraordinarily because of AI. With that, you have to train the models, target your users, understand the market dynamics, and then craft a message. All of these aspects are changing. We’re living in a time with fantastic modern tool sets for product innovation and development. You need to take advantage of these things or else your business will suffer.
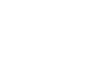
LogRocket identifies friction points in the user experience so you can make informed decisions about product and design changes that must happen to hit your goals.
With LogRocket, you can understand the scope of the issues affecting your product and prioritize the changes that need to be made. LogRocket simplifies workflows by allowing Engineering, Product, UX, and Design teams to work from the same data as you, eliminating any confusion about what needs to be done.
Get your teams on the same page — try LogRocket today.
Learn how code-style reasoning helps product managers make sharper decisions, surface edge cases, and write clearer requirements.
A practical framework for product leaders to prioritize better, reduce noise, and focus teams on what matters most.
Explore how urban planning helps product managers think in systems, strengthen foundations, and build products that scale well.
Learn how product managers can move from output tracking to outcome-driven product management with metrics tied to user impact.